ADD for All
On Big Pharma, overdiagnosis, and the questions unasked about medicalization
Americans can’t find enough Adderall. In 2021 pharmacists filled over forty million prescriptions for the popular ADHD drug, a sixteen percent increase in just two years. But this explosion in demand, likely driven by lax telehealth prescriptions during the pandemic, has run up against available supply. Because Adderall is a controlled substance, its production is carefully limited by the Drug Enforcement Agency. Some patients now ration their pills or drive hours to fill their prescriptions. People who have taken Adderall daily since they were children find themselves struggling to operate without it.
Americans find it only too easy, by contrast, to obtain methamphetamine. Of the 109,000 American drug overdose deaths last year, a third were caused by psychostimulants, mainly meth. That’s a more than tenfold increase in a decade, making methamphetamine second only to synthetic opioids, principally fentanyl, in driving the overdose crisis. This is in part thanks to meth’s new abundance and cheapness — by one estimate, illicit wholesale prices have fallen nearly eighty percent since 2016.
In many ways, the shortage of Adderall and the bounty of meth are unrelated problems. They affect different people, in different places, and at different scales. But the drugs are also chemically similar. Adderall is composed principally of the chemical amphetamine. Methamphetamine is one of many “substituted amphetamines,” substances with similar molecular structures to amphetamine. All these chemicals together form a class of drugs known as amphetamines.
There is little remarkable about the chemical amphetamine, singular, in isolation. Humans have known how to make it since 1887, when Romanian-Jewish chemist Lazăr Edeleanu first synthesized it during his doctoral studies. Edeleanu found the discovery unremarkable, just another of the hundreds of chemicals first produced in that golden age of pharmacology. In fact, it was so unremarkable that he put it aside, instead dedicating the rest of his career to the refining of crude oil. It would be another four decades before anyone thought to sell his discovery.
But when amphetamine was first marketed — in the 1930s, as the active ingredient in the decongestant inhaler Benzedrine — its social impact was immediate and profound, as Nicolas Rasmussen notes in his book On Speed: From Benzedrine to Adderall. Over the following decades, Americans embraced amphetamine, using it for everything from weight loss and cognitive enhancement to the pleasure of getting high and satisfying addiction. By 1970, nearly seven million Americans, or one in twenty adults, were using the drug by prescription alone. Including illicit use, the real total by Rasmussen’s estimate was closer to ten million.
Then, the wave hit a peak. Cocaine replaced amphetamine among swank users, while the War on Drugs decimated the street market, making amphetamine the peculiar purview of a few isolated biker gangs.
Today, though, it is back with a vengeance. About eleven million Americans aged 12 or above reported using prescription amphetamine in 2021, including three million who admitted to misuse. Two and a half million illicitly used methamphetamine.
Why have Americans picked up amphetamines again? The answer lies in a confluence of supply and demand. A culture increasingly lax about drug use again regards amphetamine as a mostly harmless wonder pill. And that demand is now fed by a modern, highly efficient supply machine, on both the licit and illicit sides of the market.
The history of amphetamine should give us pause about this new experimentation. With the return of amphetamine and its siblings has come not just death but all the highs and lows of the last crisis. As with so many other drugs, we’ve tried this one before, and found it not to our taste. A similar backlash, one suspects, is on the horizon.
America’s affair with amphetamine begins with chemist Gordon Alles. On June 3, 1929, Alles experimented on himself with fifty milligrams of the substance. Having taken his dose, Alles recorded elevated blood pressure, cleared sinuses, a “feeling of well being,” and a “rather sleepless night” during which his “mind seemed to run from one subject to another.” His friends also reported that he was a particularly ebullient dinner guest. Alles patented amphetamine for medical purposes, then sold the rights to the pharmaceutical company Smith, Kline & French for a share of the profits.
Alles and SKF had a hit on their hands. The new drug was marketed as a decongestant inhaler named Benzedrine, and in tablet form for depression and weight loss. It enjoyed widespread use on both sides of World War II. But real success came after the war, in domestic markets. In 1945, Nicolas Rasmussen estimates, domestic production was approaching three metric tons per year, “sufficient to supply half a million Americans with two tablets daily.” Production grew rapidly as Alles’s patent lapsed and other producers entered the market. In 1952, Rasmussen writes, FDA surveys indicate that production had quadrupled over the preceding three years. By 1962, it reached nearly eighty tons.
What were Americans doing with all this amphetamine? Some, of course, were using it for its indicated pharmaceutical purposes. But many more were discovering the joys of a stimulant more potent than caffeine and tobacco. Amphetamine improves energy and cognitive performance and acts as a euphoriant and aphrodisiac — hence the then-controversial 1946 song “Who Put the Benzedrine in Mrs. Murphy’s Ovaltine?” It helped that people did not really believe amphetamine to be addictive in the way that heroin was. Into the 1950s, historian Charles Jackson relates, amphetamine misuse was thought of as “a little naughty but nothing serious.”
Amphetamine even became chic. At gatherings of New York’s “Benzedrine set,” Jackson writes, “amphetamine tablets were passed out instead of cocktails.” And John F. Kennedy, America’s boy president, received regular amphetamine injections from Max Jacobson, “known as a doctor to the stars and nicknamed ‘Dr. Feelgood,’” Rasmussen writes. The Beatles had their first drug experience with Benzedrine inhalers. Millions of Americans followed these stars’ lead, taking amphetamine to help lose weight, stay energetic, and study harder.
And they didn’t always do it in the manner their doctors prescribed. “Cracking” — breaking open Benzedrine inhalers and consuming their contents — remained a popular pastime for military men and beatniks alike, delivering very large doses of amphetamine all at once. A 1960s survey of college campuses found that one in three students were using amphetamine. On four of the five campuses surveyed, amphetamine was more popular than marijuana. By 1970, Rasmussen estimates, at least ten million Americans used amphetamine. Four million sometimes used it “nonmedically,” and two million abused it.
But signs of harmful use were there almost from the beginning. In 1937, the first reports of amphetamine dependence appeared in the medical literature. In 1945, doctors stationed at one military prison observed that a quarter of inmates were cracking open Benzedrine inhalers and eating the pads inside, resulting in widespread psychosis. Amphetamine, it turned out, was not merely “a little bit naughty.” It carried with it harmful side effects and serious risk of addiction.
Amphetamines are stimulants, and stimulant abuse is generally characterized by binging, sometimes days-long repeated dosing until supply runs out or the body collapses. Long-term “speed freaks” suffered from diminished mental state, paranoia, and violent outbursts. Some high-profile crimes were connected to amphetamine users. Jackson relates the 1967 incident of an 18-year-old and a 21-year-old, both beaten and murdered in New York’s East Village while seemingly sharing meth with their assailants.
Amphetamines thus began to fall out of favor just as they came to the attention of law enforcement. The poet Allen Ginsberg, once an amphetamine user, called it “anti-social, paranoid making, it’s a drag, bad for your body, bad for your mind.” In 1970, regulations of amphetamine became stricter, making it harder to prescribe, meaning it became harder for crooked physicians to funnel pills into the black market. Desoxyn and Methedrine, both pharmaceutical methamphetamines, had been withdrawn from the market, at least temporarily: Desoxyn is today the only pharmaceutical meth on the market. The smart set, meanwhile, moved on to cocaine.
In all of this, amphetamines followed the widely recognized historical pattern of drug use. As a new drug, amphetamine entered society and was quickly embraced for its remarkable properties. The risk of addiction or harm was ignored or downplayed. It spread, finding vulnerable people, who became addicted or were otherwise hurt. Social and legal sanction followed, and, for a time, the drug faded.
The 1970s and 1980s did not see amphetamine vanish entirely. Substantially cutting off the pharmaceutical supply reduced the extent and intensity of use and abuse, but there was still some demand, and a small cadre of suppliers rose to meet it. Addiction researchers Jane Carlisle Maxwell and Mary-Lynn Brecht write that “motorcycle gangs and small-scale local producers dominated the manufacturing and distribution process,” changing their methods of production as the federal drug enforcement apparatus caught wise to each new method.
But for a long time, amphetamines lay dormant. There were local surges through the years — in Hawaii, San Diego, and Michigan’s Upper Peninsula. But for most of those two decades, America’s stimulant of choice was cocaine, first in powder form and then as crack. Amphetamine — or, even more often, meth — was something that bikers did, mostly in pockets throughout the West. In 1994, the Office of National Drug Control Policy could report that just three cities in its surveillance system — Denver, Los Angeles, and San Francisco — were seeing problems with amphetamine use, but “it has not appeared elsewhere.”
And then the problem came back. Only one year later, the ONDCP reported that “methamphetamine use appears to be spreading beyond the Western and Southwestern regions of the country” and said that the drug was “becoming more attractive to younger users.” By 1997, the ONDCP dedicated an entire section of its report to methamphetamine trends, in which it contended that the problem had been picking up steam for some time. Between 1979 and 1991, coroners had reported fewer than 100 deaths per year involving psychostimulants, a category that includes amphetamines. After that, the numbers began ticking up well into the 100s and 200s.
Part of what makes meth stand out among the drugs of that era is that it has no direct organic precursor. Cocaine, heroin, and marijuana are all derived from plants. One can make meth out of the ephedra plant, but it’s a fairly roundabout way to get there. Far more common is to source pharmaceutical precursors: for a while, producers used phenyl-2-propanone, known as P2P, but by the late ‘90s they had switched to a simple synthesis starting with pseudoephedrine, the amphetamine better known as Sudafed. While both Mexican cartels and domestic “superlabs” were major players in the market, as much as 35 percent of the meth used in the United States came from small operations that obtained their cooking knowledge from the newfangled Internet.
Because so much meth production was starting with over-the-counter pharmaceuticals, regulators had an obvious tool: crack down on the pharmaceuticals. So they did, imposing a series of controls that culminated in the 2006 passage of the Combat Methamphetamine Epidemic Act — the law that today still means that Americans must show ID when they buy pseudoephedrine for a stuffy nose. By every measure, the law was effective. Methamphetamine lab seizures peaked in 2004 at 24,000, then plummeted to 5,000. Samples of methamphetamine reported to the National Forensic Laboratory Information System also collapsed. Psychostimulant deaths peaked in 2005 at 1,600, then fell for the next three years.
But the lull did not last. As local producers were driven out, the Mexican cartels swept in to fill the void. In Mexico’s more lax legal environment, producers now source precursor chemicals from China or other underregulated countries, then convert them into plentiful, highly potent meth. In 2007, U.S. Customs and Border Protection seized one and a half metric tons of meth crossing the border. Last year, it seized eighty tons. The result of this boom, as the organization InSight Crime found, has been a remarkable drop in the wholesale price of meth, from $14,000 per pound in California twenty years ago to $1,400 today.
And with all this cheap, plentiful meth come all the harms of its widespread use. Overdose deaths began rising again in 2009. By current estimates, there were 35,000 last year. The practice of mixing meth and fentanyl into so-called “goofballs” is particularly deadly. Journalist Sam Quinones, in a 2021 Atlantic article, implicated the spread of meth in the West Coast’s ever-worsening mental health and homelessness crises.
The return of meth in the mid-1990s could, of course, just be attributed to declining taste for cocaine, or to an accident of efficiency. What makes it interesting, culturally speaking, is that it was more or less simultaneous with the return of pharmaceutical amphetamine — and with the explosion in ADHD diagnoses.
Children have been diagnosed with the symptoms we now identify as ADHD for over a century. The 1968 second edition of the Diagnostic Standard Manual of Mental Disorders included “hyperkinetic impulse disorder.” In the third edition it was renamed “attention deficit disorder,” or ADD, with and without hyperactivity. Amphetamine was used for treating patients, although the frontline treatment was methylphenidate, better known as Ritalin. But medicating kids was both controversial and relatively rare. The early 1970s saw a massive dispute over the prescription of stimulants to children, despite the relatively small number of children receiving them, perhaps two hundred thousand.
Then, in the 1990s — by which time ADD had become lumped together with ADHD as a single disorder — diagnoses began to boom. In 1997, when the CDC first surveyed the prevalence, six percent of American children were diagnosed with ADHD. Today, the figure is ten percent. The reason for the change is not perfectly clear. It may have been increased public awareness and testing, or shifts in diagnostic criteria, or both. What almost certainly fueled the trend was when, in 1991, the federal government said that students with ADHD diagnoses could receive special education services.
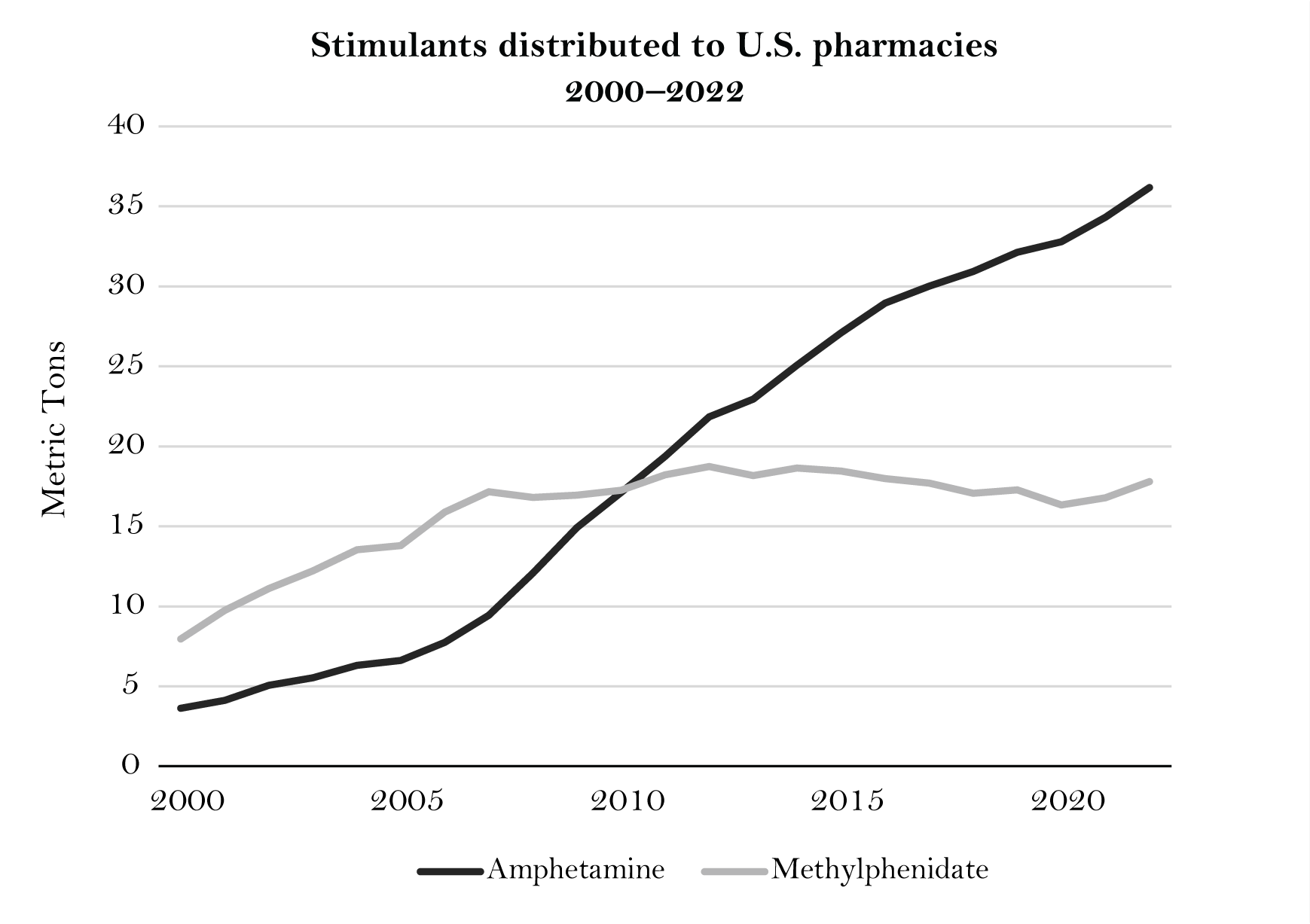
For our purposes, though, the most noteworthy change is the 1996 approval of Adderall, an amphetamine preparation, for treating ADHD. That year, there were 1.3 million amphetamine prescriptions, mainly Adderall. Just three years later, according to DEA data, the figure had risen to about 5 million. The rise of amphetamine over the following two decades may be clearest if we look at a different metric: between the years 2000 and 2022, the sheer weight of amphetamines distributed to pharmacies grew tenfold, from 3.6 metric tons to 36 metric tons. Today, Americans take more than twice as much amphetamine as Ritalin. The majority of patients are still children, but, following the conclusion in the 1990s that ADHD can persist into adulthood, a rising fraction of young adults take amphetamine too.
There are individuals who see so much improved function from taking amphetamine that prescription is appropriate. But it is hard to deny that relaxing restrictions has led to misuse. A recent study noted that rates of stimulant prescriptions in the United States grew by 250 percent from 2006 to 2016, while the rate of ADHD diagnosis only slightly increased. A 2015 analysis estimated that seventeen percent of college students were misusing stimulants, both for fun and to study harder. And on the 2021 National Survey on Drug Use and Health, respondents representing 3.7 million Americans admitted to misusing prescription stimulants in the past year.
At sufficient doses, such misuse can lead to the known harms of amphetamine abuse: psychosis, seizure, and heart attack, to name a few. But even among the population that takes amphetamine without any of these rare side effects, habituation is a growing concern. Journalist Casey Schwartz has written about the millions of young adults, herself included, who began taking Adderall to enhance their academic performance, only to find themselves unable to function, deep in withdrawal, without it. “I had long been telling myself that by taking Adderall, I was exerting total control over my fallible self,” Schwartz writes, “but in truth, it was the opposite: The Adderall made my life unpredictable, blowing black storm systems over my horizon with no warning at all.”
Everything about this pattern should be familiar. A medical regime supplies a drug that is in some cases helpful and yet remains dangerous; we ignore the harms; suffering follows. To observe this is not to say that the medical purposes are not valid, or that the tradeoff can never be worth it, but simply to acknowledge that the tradeoff exists — and to suggest that we should have been fully aware of it.
At a remove, it is easy to see the two amphetamine crises as part of the same whole. But at first blush, there are obvious differences between the amphetamine problem and the meth problem. Most users of prescription amphetamine are under 30; most methamphetamine overdose deaths are in people in their late 30s and early 40s. Amphetamine prescriptions are least common in the West, where methamphetamine overdoses are more common. Adderall abuse is a particular problem on college campuses; methamphetamine abuse is more frequent among the less educated and less well-off. It appears, in other words, that distinct populations are experimenting with the two different amphetamines.
But there does appear to be some overlap between amphetamine users and meth users. The 2021 National Survey on Drug Use and Health found that ten million Americans had misused a prescription stimulant at some point in their lives, while seventeen million had ever used meth — but those groups had three million people in common. Some advocates have floated using Adderall as a medication for meth use disorder. Reporting suggests that some people use street meth when they can’t access their amphetamine prescriptions. The two drugs, pharmacologically speaking, are not that different. While there is some evidence that meth’s chemical difference from amphetamine (namely, an added methyl group) changes its effect, it seems that the major differences are in potency, mechanism of delivery, and the social context of who uses them.
Still, anecdotal evidence of overlap does not a strong relationship make. And it is hard to argue that Adderall seeded the meth crisis, as prescription opioids seeded the fentanyl crisis. What is more persuasive is a cultural linkage: our reembrace of amphetamine, licit and illicit, points to a shift in how we relate to drugs.
One view might be that we have picked up amphetamine again because of its particular effects. This is a popular interpretation of their abuse as study drugs: kids are popping Adderall because of the ever-increasing demands of education. But that same population is using downers more too, from marijuana to opioid-laced party drugs. And the methamphetamine crisis is, of course, occurring at the same time as the ever-growing swell of opioid-overdose deaths. We seem to be using more drugs in general, not just more amphetamine.
What that suggests is a change in our comfort with drug consumption more broadly. Recall that the first amphetamine crisis took place at a time when Americans were only beginning to experiment with drugs, from new pharmaceuticals to marijuana to acid. Science produced new, wondrous substances, and their use became widespread before people started to notice harmful, sometimes deadly, side effects. Amphetamine is not the only drug for which this happened — it’s a common story, from barbiturates to psychedelics. In each case, it took decades for Americans to learn that the high was not worth the costs. And we have a habit of unlearning what prior generations learned: the cocaine and heroin problems of the 1970s and 1980s were rediscoveries of the drugs we’d tried and grown disenchanted with a century before.
Thus, the long absence of amphetamine seems to have bred ignorance of its dangers. “Nobody starts off by saying, I’m going to go develop a drug problem,” social worker Jeanette Friedman told Casey Schwartz, one of her patients. “No one means to get addicted. But there’s such a casual use of something like Adderall nowadays — because it’s seen as benign, or a help to becoming more productive.” This, of course, was also the attitude in the ‘40s and ‘50s, when amphetamine was “a little naughty but nothing serious.”
In this regard, the return of amphetamine is part of a broader reaction against the sobriety of the late twentieth century — a reaction that sweeps up everything from marijuana legalization, to the “pain revolution” that ushered in the opioid epidemic, to the new psychedelic movement. Each of these is predicated on the idea that our fears about drugs are more hype than reality. And their greatest devotees are often the relatively young, who, in addition to a greater tolerance for risk, have the least memory of what those realities are actually like.
But the story of amphetamine’s reemergence is not merely about our increased comfort with drugs. It is also about how easily those drugs can now be produced and distributed, a supply of addictive goods fueling its own demand. On the licit side of the market, the return of amphetamine has been associated with a flowering of pharmaceuticals: ADDitude magazine counts five amphetamine stimulant medications released in the sixty years before Adderall, and ten in the thirty years since. These new formulations have met ever-more-sophisticated drug marketing and prescription, particularly facilitated by the Internet. On the illicit side, too, there have been dramatic improvements in productivity, as measured by the drugs’ falling prices. Small-time meth labs have given way to the full industrial might and distributive capacity of the Mexican cartels.
Acknowledging these similarities across the licit and illicit markets may make readers uncomfortable, stuck as we may be on the idea that pharmaceutical drugs are somehow fundamentally different from those sold on the street. Amphetamine is a medicine, patients and recovery advocates insist, while methamphetamine is a dangerous drug. (Never mind that there were eight thousand prescriptions for Desoxyn, which is pharmaceutical meth, in 2021.) We even insist on distinguishing between different uses just for amphetamine: as a medication for the treatment of a disability, or as a performance enhancer or drug of abuse.
The thing is, amphetamine is all these things — therapeutic, performance enhancer, and addictive life-destroyer. The Greek word pharmakon, from which we get “pharmacology” and “pharmacy,” famously means both “poison” and “cure.” So it is with many substances. Which effect a given drug has is not constant, but varies based on many factors — the dose, the physiology and psychology of the person taking it, the presence or absence of a syndrome to which it is responding, and so on.
But while drug use is complex, the degree to which we tolerate it is in many regards not. Expanding the availability of drugs, socially and legally, expands abusive purposes along with therapeutic ones. Allowing prescription creates the possibility of misuse. More generous rules give more leverage to corrupt doctors. Tolerating a black or gray market reduces the harms of prohibition, but increases the harms of availability. Discouraging drug use reduces people’s tendency to use them, but also increases stigmatization of those who use them anyway. These tradeoffs are always present. The choice about how much we permit drug use is a choice about how much of the cost the benefit is worth, and particularly — because the risk is not evenly distributed in the population — a judgment about how much those who will suffer the costs ought to suffer so that those who will benefit can benefit.
What the return of amphetamine suggests, then, is a social shift in these preferences. Some might argue that this shift represents a desire to serve the needs of those with ADHD. But the way amphetamine prescription has outpaced ADHD diagnosis suggests that there are more “goods” being pursued than just relieving the suffering of a few. Rather, we see a willingness to prioritize some people’s joy in the high over others’ suffering in the crash. This is, of course, exactly the kind of prioritization that any market in addictive goods — from amphetamine to alcohol — looks to encourage, because it is how profits are made, whether by big pharma or the little drug pusher. In this view, the dramatic increase in drug production both responds to our social shift and further entrenches it.
If history is any indication, we will eventually learn our lesson. Americans went through one go-around with amphetamines in the postwar decades, and now we are doing it again. Drugs come and go in cycles, and at some point we will decide that letting tens of thousands die, and putting millions of children on drugs for life, comes at a cost we no longer wish to bear. But we are not there yet. And there is little sign we will be there for some time to come.
Exhausted by science and tech debates that go nowhere?